|
Addressing Behavioral Health Needs of Men: Substance Abuse > Chapter 4 - Working With Specific Populations of Men in Behavioral Health Settings
|
|
 4. Working With Specific Populations of Men in Behavioral Health SettingsIntroductionThe patterns of substance abuse and the treatment needs of adult men (ages 18 and older) are diverse, as are their conceptions of masculinity. Men in need of treatment come from all walks of life;this chapter outlines some of the patterns of substance use and abuse for specific populations of men, noting areas in which men differ from women. Clinical examples and tips are offered to guide behavioral health clinicians in treating men from these diverse populations.
Men With Co-Occurring DisordersMany men in treatment for a substance use disorder have a co-occurring mental disorder. In the general population, men are less likely to have serious mental illness than women (Epstein et al.2004), but a larger percentage (56 percent) of adults in substance abuse treatment with co-occurring mental disorders are men, just as more adults in substance abuse treatment overall are men (Office of Applied Studies [OAS] 2004 a). Among adults with serious mental illness, men are more likely than women to have used illicit substances in the past year (Epstein et al. 2004; Substance Abuse and Mental Health Services Administration [SAMHSA], OAS 2007a).
[Question #77. Many men in treatment for a substance use disorder have a co-occurring mental disorder true/false?] Men with co-occurring disorders are more likely than women with co-occurring disorders to use more than one illicit substance and are more likely to report daily use of illicit substances (SAMHSA,OAS 2007 a). Data from 2003 show that, as a group, men with co-occurring disorders are more likely to have dropped out of high school than their female counterparts (17 percent of women versus 28 percent of men), less likely to have health insurance (77 percent of women versus 67 percent of men), and less likely to have received treatment for substance abuse or a mental disorder in the past year (55.4 percent of women versus 41 percent of men) (OAS 2004b). As noted in Chapter 1, men are more reluctant to seek professional assistance for health-related problems, including substance abuse and mental illness, than women (Addis and Mahalik 2003; Grella et al. 2009a). Therefore, although people with co-occurring disorders are more likely to seek mental health services than those with just a substance use or mental disorder (Wu et al. 1999), a large number of men with co-occurring disorders still seek no treatment for either disorder. Masculine gender norms can cause men to feel greater shame than women in seeking help for mental illness (Addis and Mahalik 2003). The “Counseling Men Who Feel Excessive Shame” section in Chapter 3 of this Treatment Improvement Protocol (TIP) addresses shame related to the failure to meet masculine gender expectations and offers advice on addressing shame. Even men already in substance abuse treatment may be reluctant to seek assistance with co-occurring mental disorders, so programs that work with male clients need to be especially proactive in screening and assessing such disorders (see Chapter 3) and assisting these clients in getting the help they need. Conducting a thorough medical and mental health assessment at admission can minimize the risk of these disorders going untreated, even if the program itself cannot provide that treatment.Screening and assessment for mental illness must also be ongoing; clients with one type of disorder are at increased risk of later developing disorders of another type. Moreover, the symptoms of a substance use disorder can mask co-occurring mental disorder symptoms at any point in treatment.Treatment Improvement Protocol (TIP) 42, Substance Abuse Treatment for Persons With Co-Occurring Disorders (Center for Substance Abuse Treatment[CSAT] 2005c), details the screening, assessment, and treatment of co-occurring disorders in male and female clients and offers information on various co-occurring mental disorders (some of which are discussed later in this TIP). Chapter 5 of TIP 42 presents strategies for treating people with co-occurring disorders. When screening for co-occurring disorders(see advice box below), clinicians may find that many men are uncomfortable discussing the emotional aspects of mental illness and will focus more on tangible symptoms, such as difficulties in sleeping, changes in appetite,physical complaints, decreased interest in sex).For this reason, male clients with co-occurring disorders may be less interested in psychotherapy than female clients. Male clients may also present with more behavioral problems than women (e.g., fighting, lack of compliance with medication regimen). Advice to Behavioral Health Clinicians: Screening and Assessment for Co-Occurring Disorders in Men
Anxiety DisordersIn general, men are less likely to have anxiety disorders than women (American Psychiatric Association [APA] 2000; Grant et al. 2009;Kessler 1998). The only exceptions are social phobia and obsessive–compulsive disorder(OCD), as some research has found that rates for those do not vary significantly between genders (Bekker and van Mens-Verhulst 2007;Grant et al. 2009).
[Question #55. The rate for occurrence do not vary significantly between genders in] However, rates of anxiety disorders among men with substance use disorders vary from those found in the general population. For example, OCD appears to be much more common among persons with substance use disorders (see discussion later in this chapter).Rates also vary according to treatment setting and primary substance of abuse. Even within a specific type of setting, rates vary greatly according to the assessment instruments used and other factors. For example, a study of men who were incarcerated and receiving substance abuse treatment found that 17.8 percent had met criteria for an anxiety disorder at some point during their lives (Zlotnick et al. 2008),whereas another study of men entering the prison system found that 74.6 percent met criteria for a current substance use disorder and 36.4 percent met criteria for a current anxiety disorder (Gunter et al. 2008). Other research comparing rates of anxiety disorders among individuals with different substance use disorders has found significantly higher rates in those with cocaine use disorders (Conway etal. 2006; McRae et al. 2007). One significant issue for men with co-occurring anxiety and substance use disorders is the use of alcohol and/or drugs to cope with anxiety symptoms (sometimes called self-medication). Robinson and colleagues (2009) evaluated data from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), which surveyed over 43,000 adult men and women and inquired about alcohol and/or drug use to reduce symptoms associated with specific anxiety disorders.They found that the frequency of this behavior varied depending on the type of anxiety disorder a person had; 35.6 percent of men and women with generalized anxiety disorder(GAD) reported self-medicating, but only 7.9 percent of those with social phobia did so. Men with anxiety disorders were significantly more likely to report such behavior than were women with anxiety disorders. For men with co-occurring anxiety and substance use disorders, substance abuse may be a means of coping, but as the substance use disorder progresses, it actually worsens anxiety disorder symptoms. Substance abuse treatment is complicated by subsequent patient resistance toward giving up a drug that he feels is necessary for his emotional survival, by anxiety arising from emotionally intense treatment, and, in some cases, by deficits in social skills important in substance abuse recovery.Because of masculine social norms, men may feel greater pressure to deny anxiety or to use avoidance coping methods (such as self-medication) to address it.This behavior can bea persistent problem that endangers recovery for men with anxiety disorders, and it serves as an added impetus for counselors to address anxiety in treatment. The following sections examine anxiety-related mental health issues commonly seen among men in substance abuse treatment, including posttraumatic stress disorder (PTSD), social phobia, OCD, GAD, and combat stress reaction (CSR). [Question #57. Anxiety-related mental health issues commonly seen among men in substance abuse treatment are:] Posttraumatic stress disorderIn the general population, men are exposed to trauma more often than women, although women experience higher rates of PTSD(Breslau 2002; Kessler et al. 1995). Between 5and 6 percent of men have had PTSD sometime in their lives (Breslau et al. 1998; Kessleret al. 1995). However, in certain male populations exposed to greater amounts of trauma,rates of PTSD are likely to be higher. Studies have found rates of trauma exposure between 42 and 95 percent in men seeking treatment for substance use disorders (Farley et al. 2004)and equally high rates in populations of men with serious mental illness (Goodman et al. 2001) and men who are homeless with co-occurring disorders (Christensen et al. 2004).Men involved in the criminal justice system (Swartz and Lurigio 1999) and men who are combat veterans (Kulka et al. 1990) are 2 to 3 times more likely to experience PTSD than men in the general population.
Prior trauma exposure may also contribute to the development of PTSD following a subsequent trauma. Smith and colleagues (2008)report that individuals who had been the victim of an assault prior to being deployed in Operation Iraqi Freedom (OIF) were twice as likely to develop new-onset PTSD during or after deployment than were service members with no history of assault. Kessler and colleagues (1995) found that men with PTSD are more likely to have a co-occurring substance use disorder (51.9 percent) than men without PTSD (34.5 percent) and are also more likely to have a co-occurring substance use disorder than women with PTSD (27.9 versus 26.9 percent, respectively). These data suggest that men in substance abuse treatment are at particularly high risk for having both PTSD and a substance use disorder. Men and women are typically exposed to different types of trauma and appear to be affected differently by traumatic events. The most common traumas for men are exposure to combat; being physically assaulted, shot, or stabbed; and witnessing killings or serious injuries. Women, however, are most often exposed to sexual assault and rape (Breslau 2002;Kessler et al. 1995). Men are also more likely than women to be victims of violent crime (Catalano 2004). In a sample of men with substance use disorders (both in and out of treatment), 45 percent had witnessed a killing or injury, 33 percent had been physically assaulted, 16 percent had been threatened, and 16 percent had experienced a sudden injury or accident; women were 14 times more likely to have been raped than men but 3 times less likely to have been physically assaulted(Cottler et al. 2001). Among men, rape and combat are the two types of trauma most likely to lead to PTSD.In a general population sample of men, rape (a relatively rare event for adult men) resulted in PTSD approximately 65 percent of the time; combat exposure resulted in PTSD 38.8 percent of the time (Kessler et al. 1995). [Question #56. Among men, rape and combat are the two types of trauma most likely to lead to :] Men are expected to be tough, so their trauma histories may not be explored in treatment as often as those of women, nor are they as likely to self-identify as trauma survivors. The problem is complicated by men’s greater tendency to externalize their experiences of trauma; thus,men are more likely than women to react to their own traumatization by victimizing others.Men are also more likely to report symptoms of increased alcohol use and irritability as a result of traumatic experiences (Green 2003). Case example: Tim Tim is a 30-year-old veteran of OIF. While on active duty, he was exposed to several life-threatening events, including being in a convoy vehicle that hit an improvised explosive device (IED) on the roadside. The passenger in the vehicle’s front seat was killed, and Tim was thrown from the back, resulting in abrasions and bruises across his body, a broken arm and knee cap, and wounds from shrapnel. At the time of this traumatic event, Tim was screened for trauma symptoms but was approved to return to combat; as soon as his wounds healed, he returned to his unit for another 7 months of active duty. Following his discharge from the Army, Tim entered college and majored in criminal justice. Although he had exhibited some trauma symptoms prior to starting college (sleep disturbances, nightmares, anxiety when he saw objects on the side of the road), the symptoms were not disabling until he began an internship at a local prison. Within the first month of the internship, Tim began experiencing disabling PTSD symptoms that were exacerbated by the noises, sights, and smells in the prison.The yelling among inmates and the clanging of metal doors were particularly stressful. He began smoking marijuana after work and on weekends to quell his symptoms, and he tested positive for marijuana on a routine drug screen.He was referred to the prison’s employee assistance program, which referred him to a substance abuse treatment program for evaluation. The substance abuse program staff identified Tim’s co-occurring PTSD and substance abuse and enrolled him in a 2-month assessment group for his substance use. To address his PTSD symptoms, the program also arranged regularly scheduled appointments at the local U.S. Department of Veterans Affairs (VA) clinic with a behavioral health counselor who had been trained in PTSD treatment. The planned TIP, Trauma-Informed Care in Behavioral Health Services (SAMHSA planned g), provides more information on trauma and PTSD among men and women with substance use disorders and on treating trauma concurrently with substance use disorders. It offers more detail regarding all trauma-related subjects touched on in the following sections of this chapter. Treating men for PTSD Many interventions to address both PTSD and substance use disorders, even if developed for both male and female clients, have been evaluated primarily with women or with men who have experienced combat-related trauma.Behavioral health clinicians may need to consider how to adapt these interventions for other populations. In some cases, models created specifically for women have been adapted for men; one such example is the Men’s Trauma Recovery and Empowerment Model (MTREM). This model appears promising in its ability to engage male clients and improve their coping skills, and it is a useful example of how trauma treatment can be adapted for a male population (personal communication with R. D. Fallot, June 10, 2005). However,research on M-TREM’s effectiveness is ongoing; no recent study reports are available to provide empirical evidence of its potential success. [Question #58. The trauma treatment model to engage male clients and improve their coping skills is:] The developers who adapted TREM for male clients formulated eight basic assumptions about how trauma treatment for men should differ from that provided to women. These assumptions are shown, along with the developers’ responses to them, in Exhibit 4-1. 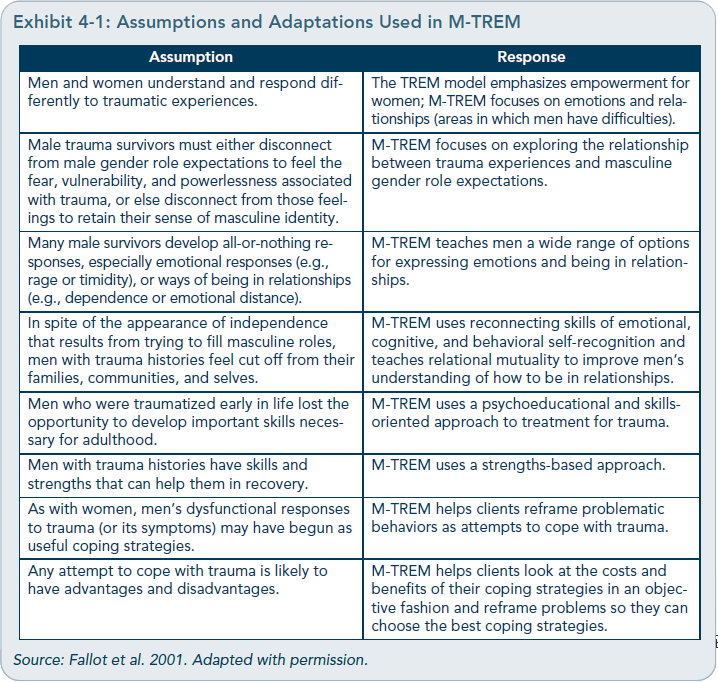 Other researchers and behavioral health clinicians have suggested ways in which treatment for men with PTSD may need to differ from that provided for women with the disorder.For example, Lisak (2001b) notes that the ideology of masculinity limits the resources available to men to respond to trauma. Therefore,any treatment for men with trauma must address how men internalize masculine ideology concurrently with their trauma histories. Otherwise, the legacies of masculine socialization can impede the process of healing from trauma by keeping men from connecting with the painful feelings that result from it.
Ruzek (2003) describes several interventions for treating veterans with co-occurring PTSD and substance use disorders; most of this population is male, and the research Ruzek draws upon is primarily with male clients. Specifically, he notes that members of this population often have anger control problems that need to be addressed in the context of their trauma treatment. The Seeking Safety model for treating co-occurring trauma and substance use disorders effectively reduced PTSD symptoms and substance use in a small (n=5) study of men with co-occurring substance use disorders and PTSD (Najavits et al. 2005). Emotionally directed, cognitively oriented counseling can help men connect with their feelings and the feelings and experiences of others (Hardy 2004). Treatment for trauma and trauma-related disorders typically involves the active processing of painful feelings that expose the individual as vulnerable—an exploration that runs counter to the masculine norms of our culture, thus making this process potentially more difficult with male clients than with female clients. Because of this added impediment, behavioral health clinicians treating men with trauma histories must explore with them the social processes of masculinization and the ways in which masculine norms hinder recovery from trauma (Lisak 2001b). Treatment for men with histories of trauma, whether or not they have PTSD, is discussed later in this chapter. Specific information on treating men exposed to combat trauma is presented in the following section. Combat stress reactionCSR is an acute anxiety reaction similar to an acute stress disorder but only occurring among combatants (and noncombatants exposed to combat events) in an armed combat situation.Although the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition,Text Revision (DSM-IV-TR; APA 2000) does not list CSR as a diagnosis, CSR (also called combat trauma) affects a significant number of male veterans. Substance use and mental disorders are strongly associated with trauma from combat exposure (Hoge et al.2006; Ruzek 2003).
[Question #60. The treatment reference for mental health issues among veterans is:] [Question #59. An acute anxiety reaction similar to an acute stress disorder but only occurring among combatants is:] Common causes of CSR often relate to direct attacks, as with insurgent small arms fire or IEDs, and can also result from being near combat, handling the bodies of wounded or dead individuals, being repeatedly exposed to events with a high risk of death or injury, or making frequent on-the-spot decisions under ambiguous conditions—especially when the result is death or injury to others. CSR can be transient and nondebilitating, orit can result in major psychological disorganization. Normally, with support and treatment,symptoms diminish in a relatively brief period of time (1 to 2 months). If symptoms persist beyond that time, the person may be diagnosed with PTSD. Typical CSR symptoms include hyper vigilance, sleeplessness, irritability, anger, and difficulty concentrating. More severe symptoms may include freezing up,feelings of impending doom, significant but unreasonable guilt, unpredictable responses in ordinary situations, and impaired memory. Significant strides have been made in recent years in addressing CSR in combat zones.Military personnel are briefed prior to entering a war theater about stressors and coping strategies. Personnel with combat stress symptoms are more rapidly and efficiently identified, and onsite treatment in the combat zone has been remarkably improved. Most treatment for service members is provided in their assigned camp by members of combat stress control teams composed of behavioral health professionals who use brief and targeted individual, group, and psychoeducational methods.If service members do not respond to these services, they are evacuated from the combat zone whenever possible to access more specialized resources. A more detailed deblockedion of this process is described in the planned TIP, Trauma-Informed Care in Behavioral Health Services (SAMHSA planned g). Reintegration efforts for veterans returning to the United States have been significantly enhanced as well. Programs for families, ongoing medical care, and civilian life have been developed and implemented throughout all service branches. Behavioral health clinicians should know that veterans are eligible for a variety of services offered by regional VA centers, including readjustment counseling, referral for benefits assistance, marital and family counseling, substance abuse information and treatment referral, job counseling and vocational assistance referral, and sexual trauma counseling and treatment referral. The Iraq War Clinician Guide (National Center for PTSD and Walter Reed Army Medical Center 2004) is a treatment reference for mental health issues among veterans of OIF. This document is available for free on VA’s National Center for PTSD Web site (http://www.ptsd.va.gov/professional/manuals/manual-pdf/iwcg/iraq_clinician_guide_v2.pdf). Military One Source also offers veterans and their families useful resources relating to mental health and substance abuse issues (http://www.militaryonesource.mil; 1–800–342–9647). Social phobiaSocial phobia, also called social anxiety disorder, is one of the most common anxiety disorders. It affects women more than men, with a lifetime occurrence of 15.5 percent for women and 11.1 percent for men (APA 2000; Kessler1998). It entails a “marked and persistent fear of social or performance situations in which embarrassment may occur” (APA 2000, p.450). Men with social phobia seek treatment more often than women, which is opposite the norm for most mental disorders (Weinstock 1999). Men may be more likely to seek treatment for this disorder because it has a greater impact on them due to the gender role expectation that they be more proactive in social relations.
[Question #61. Women with social phobia seek treatment more often than men.true/false?] Men are particularly susceptible to using alcohol to combat the symptoms of social phobia.Some men describe how they drink to be able to leave the house, interact with others, or work in front of others (e.g., when making presentations). Men with social phobia may use alcohol at work when confronted with stressors that involve interpersonal interaction.They may drink heavily at unavoidable social events and then experience the negative effects of heavy use. Social phobia also makes it difficult for men to enter substance abuse treatment, where they fear being overwhelmed with anxiety. They may be especially fearful of group sessions or 12-Step participation and will feign illness or other crises to avoid attending. It can be easy for counselors to equate this behavior with clients being resistant or less motivated. Many clients with social phobia have anticipatory anxiety: imagining a worst case scenario about an upcoming event at which they might be the center of attention, interrogated by others, or exposed as a fraud; they then react emotionally as if that event has occurred.Anticipatory anxiety emotionally validates that the upcoming event is, indeed, dangerous and needs to be avoided. Some people cope with anticipatory anxiety by using drugs or alcohol to quell their symptoms. [Question #62. Clients imagining a worst case scenario about an upcoming event at which they might be the center of attention have:] Screen clients with social phobia symptoms (see DSM-IV-TR for symptoms; APA 2000) for the disorder and refer, if necessary, to qualified behavioral health professionals who specialize in the treatment of anxiety disorders for assessment and discussion of treatment options, including counseling (especially cognitive–behavioral therapy) and medication.Along with confronting limiting beliefs and perceptions, counseling should build skills in social interaction, anxiety self-monitoring, and positive coping options for use during anxiety-producing social situations. Obsessive–compulsive disorderAlthough not highly prevalent in the general population, OCD almost always co-occurs with other mental disorders and often with substance use disorders (Mancebo et al. 2009;Pinto et al. 2006). A study of people in treatment for OCD found that 27 percent of the sample met criteria for a lifetime diagnosis ofa substance use disorder; men were more likely than women to have a co-occurring substance use disorder.
For a man with OCD and a co-occurring substance use disorder, the substance use disorder may have originated in an attempt to cope with overwhelming and disabling anxiety.However, as substance use progresses, it actually worsens anxiety symptoms. Substance abuse treatment can be complicated by men’s resistance to giving up a drug that they believe necessary to their emotional survival, by anxiety that arises from the emotional intensity of treatment, and sometimes, by deficits in social skills important for recovery from substance abuse. As with other anxiety disorders, a licensed behavioral health service provider with specific training in the treatment of anxiety disorders should diagnose and treat OCD, which should be treated concurrently with the substance use disorder. In addition to counseling, treatment may include medication. Generalized anxiety disorderGAD is sometimes associated with substance use disorders. In cases of GAD, the origins of the substance use disorder may lie in attempts to cope with overwhelming and disabling anxiety. However, as substance use progresses, it actually worsens anxiety symptoms. Substance abuse treatment can be complicated by men’s resistance to giving up a drug that they believe necessary to their emotional survival, by anxiety that arises from the emotional intensity of treatment, and sometimes, by deficits in social skills important for recovery from substance abuse. As with other anxiety disorders, a licensed behavioral health service provider who specializes in the treatment of anxiety disorders should conduct diagnosis and treatment;the anxiety disorder needs to be treated concurrently with the substance use disorder.
Mood DisordersIn general, women are more likely to experience mood (i.e., affective) disorders than men(APA 2000; Kessler et al. 1994), although the reasons for this difference are unclear. The same factors that protect men against certain disorders may contribute to increased rates of other disorders or problems, such as an increased rate of death by suicide among men(see the “Suicidality” section starting on p. 81). Furthermore, affective disorders may be more common in men than is generally believed,due to under diagnosis or misdiagnosis (Levinand Sanacora 2007). Mood disorders can present with a wide range of symptomatology.Some of the more common mood disorders seen in substance abuse clients include dysthymia, a chronic depressed mood that extends over years; major depressive disorder, which manifests as recurring, significantly disabling depressive episodes; bipolar disorder, which can manifest as recurrent, interspersed manic and depressive episodes; and cyclothymia, which comprises cyclical manic and depressive episodes that do not meet criteria for bipolar disorder or substance-induced mood disorder. For more information on assessment and treatment of these disorders, see TIP 48, Managing Depressive Symptoms in Substance Abuse Clients During Early Recovery (CSAT 2008b).
Dysthymia and major depressive disorderAccording to a number of studies, women are from 1.5 to 3 times as likely as men to have a depressive disorder, and this finding holds true in many settings around the world (Chuick etal. 2009; Kessler 2000a; Levin and Sanacora2007). However, approximately 12.7 percent of all men will experience an episode of major depression at least once during their lives (Kessler et al. 1994).
Different explanations have been proposed for the large difference in rates of depression between genders. Depression seems to manifest differently in men than in women.This may contribute to the higher incidence of substance use disorders and antisocial personality disorder(ASPD) in men than women (NationalInstitute of Mental Health [NIMH] 2003; Pollack 1998c; Real 1997). Others have suggested that the apparent difference may exist because men are less likely to seek help for depression, present with different symptoms of depression than women, and may be diagnosed by behavioral health clinicians and diagnostic instruments that are influenced by gender bias. Men tend to be underdiagnosed with depression, whereas women are overdiagnosed (Levin and Sanacora 2007). However,conclusive evidence supporting a single explanation is still lacking (Winkler et al. 2004). The fact that men are less often diagnosed with depression than women may also result from cultural factors that define permissible masculine behavior—so that the same gender roles that shield men from their emotions in other areas may keep them from showing symptoms of depression, alter their symptoms,or make them less likely to report symptoms. Studies also show that rates of depression are nearly the same among some subgroups of men and women, such as the elderly (Bebbington et al. 2003) or certain cultural/ethnic groups (e.g., the Amish, HassidicJews), in which men are less likely than men in the general population to have substance use disorders, ASPD, or other problems that may be manifestations of underlying issues thatalso cause depression (Cochran 2001). A study of patients at a German hospital found gender differences in the presentation of symptoms, but not the severity, of depression—with men who were depressed more likely to show emotional rigidity, blunted affect, and decreased libido (Winkler et al.2004). Men who are depressed may be more likely to focus on somatic or physical complaints than women, and depression in men may manifest in interpersonal difficulties andconflicts. Notably, men with depression are more likely to have a substance use disorder than women who are depressed (Cochran2001; Pollack 1998c). Depressed mood, whether attributable to aspecific disorder or not, can significantly affect substance abuse treatment and recovery. For example, among a group of men who had relapsed during the 12 months following treatment, the most reported reason for relapse—reported by 26.9 percent of participants—was depressed mood (Strowig 2000). Such feelings as boredom and anger can cause relapse to substance use and may also result from underlying depression. TIP 48 (CSAT 2008b) discusses how to address subclinical depressive symptoms (for men and women) in substance abuse treatment settings. Treatment for depressive disorders can be concurrent with substance abuse treatment. It usually includes a combination of counseling and antidepressant medication, which only behavioral health clinicians specifically trained in the treatment of mood disorders should provide. The Nature of Depressive SymptomsThe term “depressive symptoms” is generally applied to a state of sadness, depressed mood, the blues, or related feelings and behaviors that do not meet diagnostic criteria for a DSM-IV-TR (APA 2000) mood disorder. People with such symptoms may experience considerable emotional pain and significantly impaired functioning in some areas.
Symptoms of depression exist on a continuum ranging from sadness and other depressive symptoms occurring at appropriate times and for short periods, during which the individual successfully uses coping strategies, to clinical (or major) depression as described in the DSM-IV-TR (APA 2000). The line between depressive symptoms and full-blown depressive disorders is a question of degree. Having depressive symptoms differs from having a major depressive disorder in terms of the number or severity, but not the type, of symptoms experienced by a client. Only behavioral health professionals credentialed to diagnose mental illness can determine whether a client has a serious disorder, such as major depression, dysthymia, bipolar disorder, or substance-induced mood disorder. Counselors who suspect that a client has a depressive illness should refer him to a behavioral health professional for assessment, diagnosis, and treatment. Depressive symptoms may become more or less intense over time due to the client’s physiology, stressful events in the client’s life, or the client’s stopping or starting substance use. For example, someone who drinks heavily may have intense depressive symptoms that seemingly meet criteria for depressive illness but lessen dramatically in the weeks after initial abstinence from alcohol. Similarly, someone with major depression or dysthymia who has taken antidepressant medication for several weeks may show few or no currently debilitating depressive symptoms. Conversely, a client may demonstrate only mild depressive symptoms at intake but may be headed toward a significant depressive episode. As with substance abuse, although a person may be in remission from his depressive symptoms, the depressive disorder may remain. Treatment must address prevention of and early intervention in recurrences, especially during early recovery from substance use disorders. Many depressive disorders cycle and recur. If a client has a history of a mood disorder, he and his counselor should be on the lookout for a recurrence of symptoms. Source: CSAT 2008b, page 5. Adapted from material in the public domain. Bipolar disorderMen and women appear to be affected differently by bipolar disorder.The disorder has an earlier age of onset in men than in women;men with the disorder also seem to have more frequent manic episodes and require a greater number of weeks of hospitalization for these episodes than women with the disorder,whereas women have more depressive episodes than men (Arnold 2003). Men with bipolar disorder appear more likely than women with the disorder to have a co-occurring substance use disorder, according to a number of studies reviewed by Arnold (2003); see also Albanese and colleagues (2006).
Many clients in substance abuse recovery who have been diagnosed with bipolar disorder describe trying to regulate their manic and depressive cycles with substances. For instance, in a manic episode, clients may use alcohol or sedatives to sleep and/or stimulant drugs to increase the high of the episode (i.e., emotional expansiveness and sense of well-being). In a depressive cycle, clients may use alcohol (even though it is a depressive drug) to dull the pain of their depression and/or stimulants to counteract the effects of the depression. [Question #63. In a depressive cycle, clients may use alcohol as a depressive drug to dull the pain of their depression and/or stimulants to counteract the effects of the depression true/false?] depression. Manic symptoms can often be confused with symptoms of substance abuse, making diagnosis simply by observation difficult. Generally,bipolar disorder has to be diagnosed by a thorough examination of the client’s mental health history, which should be conducted by a licensed behavioral health professional trained in making such diagnoses. Treatment for the substance use and bipolar disorders needs to be integrated or at least concurrent, as symptoms for one can trigger onset or relapse of the other. In addition to counseling, psychotropic medication is usually prescribed to regulate the bipolar disorder; the use of medication to regulate the illness must be considered in the client’s total treatment plan. SchizophreniaAcross cultures, the onset of schizophrenia begins earlier in men than women (Moriarty et al. 2001; Nasser et al. 2002). The DSM-IVTR (APA 2000) notes that the age of onset of schizophrenia is typically between 18 and 25 years of age for men and between 25 and the mid-30s for women. Some research suggests gender differences in the course and presentation of schizophrenia as well. In diagnosing schizophrenia, clinicians look for positive symptoms (i.e., an excess or distortion of normal function) and negative symptoms (i.e., a decrease in or loss of normal functions). Men appear to have more severe negative symptoms (e.g., emotional withdrawal, lack of spontaneity, blunted affect) and less severe positive symptoms (e.g., hallucinations, delusions) than women with schizophrenia (Moriarty et al.2001). Men with the disorder also seem to have higher rates of co-occurring substance use disorders than women with schizophrenia(Fowler et al. 1998). One large-scale study of1,027 veterans with schizophrenia (97 percent male) found that more than half had a history of substance abuse (Bailey et al. 1997).
Men with schizophrenia typically have poorer treatment outcomes than women (Moriarty etal. 2001), and they do not always respond as well as women to medications or to family involvement in treatment. Haas and colleagues (1990) found that an inpatient psychoeducational intervention for clients’ families was associated with improved symptoms and functioning in women but with worsened symptoms and functioning in men.The effectiveness of family involvement depends on how the family is involved. In reviewing three studies, Ayuso-Guiterrez and del Rio Vega(1997) found significantly reduced relapse rates for clients with schizophrenia whose families received psychoeducational or behavioral interventions. Women with schizophrenia may respond better to certain medications than men (Goldstein et al. 2002), but this may be due to better medication compliance in women (Nasser et al. 2002). Some symptoms of schizophrenia may be masked by drug use, which can cause the schizophrenic illness to be overlooked—particularly among young men in whom the illness is just emerging. Symptoms, such as blunted affect and other negative symptoms,poor interpersonal relationships, and poor self-care, may be seen as by-products of drug use,with the expectation that these symptoms will improve with abstinence. However, with schizophrenic illness, only temporary remission is typically seen, and the symptoms may even appear more pronounced with drug abstinence. Careful mental health evaluation is required for differential diagnosis and treatment planning. Pathological GamblingPathological gambling is an impulse-control disorder characterized by “persistent and recurrent” gambling “that disrupts personal, family,or vocational pursuits” (APA 2000, p. 671).Two thirds of individuals with this disorder are men, in whom it typically begins at an earlier age (early adolescence) than in women(APA 2000). Men are more likely than womento be in treatment for pathological gambling or to attend Gamblers Anonymous (Ladd andPetry 2002; LairRobinson 1997). In fact, theDSM-IV-TR estimates that 96 to 98 percent of people in treatment for this disorder are men (APA 2000). Men who gamble pathologically are significantly more likely than men inthe general population to have a co-occurring substance use disorder (Kessler et al. 2008;Scherrer et al. 2007).
[Question #64. An impulse-control disorder characterized by persistent and recurrent gaming that disrupts personal, family, or vocational pursuits is:] Pathological gambling is more common among people with substance use disorders than among those who do not have such disorders. One study of 113 patients admitted to a gambling treatment program found that 66.4 percent had a lifetime incidence of a substance use disorder (Kausch 2003). Other researchers have found equally high or higher levels of co-occurring substance use and pathological gambling disorders, and problem gamblers who have alcohol use disorders may also have more severe gambling problems than those who do not abuse alcohol (Stewart and Kushner 2003). In a study of gambling treatment program admissions, gamblers with substance abuse treatment histories had more severe gambling problems than other participants, including greater number of years with a problem and greater number of days spent gambling in the month prior to treatment entry (Ladd and Petry 2003). Other risk factors for pathological gambling include lower socioeconomic status (SES), gambling at casinos,and participating in a greater number of different games of chance (Welte et al. 2004).Appendix D of TIP 42 (CSAT 2005c) addresses pathological gambling in clients with co-occurring substance use disorders. Eating DisordersBecause of the relative rarity of eating disorders among men, many clinicians may not expect to see or may not recognize eating disorders in their male clients. However, studies show prevalence rates of bulimia in men from 0.1 percent to 2.1 percent (Makino et al.2004). Two studies that administered the Eating Attitudes Test-26 found that 4 and 10 percent of the men in their respective samples had abnormal eating attitudes (Makino et al.2004). General population studies have not measured the prevalence among men of anorexia nervosa (the other specifically diagnosable eating disorder). However, a study of 135 men with diagnosable eating disorders who were treated at a Boston hospital found 22percent to be anorexic and 46 percent to bebulimic; 32 percent had an unspecified eating disorder (Carlat et al. 1997).
A study by Carlat and colleagues (1997) found that 37 percent of men with eating disorders had a co-occurring diagnosis of substance abuse or dependence. A large percentage of the men sampled were gay or bisexual: 27 percent of the total and 42 percent of the men with bulimia. Eating disorders are often related to poor body image (Shelton and Liljequist2002), which is also associated with increased alcohol use and physical and verbal aggressiveness. Given these data, clinicians should expect to see men in treatment for substance use disorders who also have eating disorders,and they should be prepared to screen for these disorders and refer clients for treatment when warranted. TIP 42 (CSAT 2005c) explores the treatment of clients who have co-occurring substance use and eating disorders. Even men who do not meet criteria for an eating disorder may develop disordered eating practices (e.g., binge eating, eating to regulate mood) in early recovery, and men in later recovery may feel distress about weight gain that occurs after they stop using substances (Cowan and Devine 2008). Personality DisordersThe DSM-IV-TR (APA 2000) describes 10 different personality disorders, some of which seem to affect women more than men (i.e., border line personality disorder, dependent personality disorder), some of which seem to affect the genders about equally (i.e., histrionic personality disorder, avoidant personality disorder), and some of which appear to affect men more than women (i.e., paranoid personality disorder, schizoid personality disorder,schizotypal personality disorder, ASPD,narcissistic personality disorder, obsessive compulsive personality disorder [OCPD]).The greatest gender differences are in ASPD,which affects at least three times as many menas women in the general population; OCPD,which affects twice as many men as women;and borderline personality disorder, which affects about three times as many women as men (APA 2000).
Recent epidemiologic research paints a somewhat different picture of the prevalence of personality disorders. NESARC, which surveyed over 43,000 adult men and women, found that OCPD was the most common personality disorder (affecting 7.9 percent of the population) and was about equally common for men and women. The survey excluded borderline,schizotypal, and narcissistic personality disorders because of the greater number of questions needed to assess for those disorders (Grant et al. 2005). Grant and colleagues (2004b) reviewed NESARC data and found that avoidant, dependent, and paranoid personality disorders were significantly more common among women than men, but that men were more likely to have ASPD. They investigated the rates of co-occurring personality and substance use disorders and found that co-occurring personality disorders were much more common among people with drug use disorders (47.7 percent) than among people who had alcohol use disorder (28.6 percent).Exhibit 4-2 depicts rates of co-occurring personality disorders among men with substance use disorders (Grant et al. 2004b). 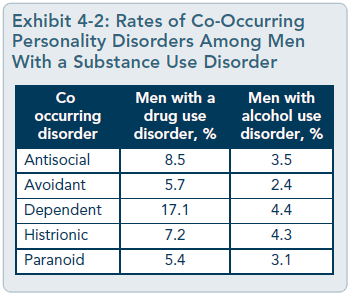 Antisocial personality disorderThe National Comorbidity Study found that 5.8 percent of men (compared with 1.2 percent of women) had sufficient symptoms to warrant a diagnosis of ASPD at some point during their lifetimes (Kessler et al. 1994).NESARC found similar rates of 5.5 percentfor men and 1.9 percent for women (Grant etal. 2004b). In a study by Klonsky and colleagues (2002), ASPD was associated with both self-endorsement of masculine attributes and peer reports of masculine attributes among a sample of male and female college students. In large-scale studies, 80 percent of ASPD cases in the general population are men; this may relate to impulsive aggression,which characterizes ASPD, being a trait more common to men than women (Paris 2004).Most ASPD symptoms are described in terms of male behavior, so women may be underdiagnosed if they have ASPD symptoms less likely to appear in diagnostic criteria, such as stealing from an employer or engaging in prostitution.
[Question #65. Community alternative treatment programs for co-occurring Antisocial personality disorder (ASPD), often found in prison, are:] Studies of people in substance abuse treatment(Compton et al. 2000) and people with substance use disorders who are not in treatment (Falck et al. 2004) have found much higher rates of ASPD for both men and women. Moreover, rates of ASPD in treatment settings tend to be closer between genders than rates found in the general population (Millery and Kleinman 2001), and some researchers have even found slightly higher rates among women in treatment than among their male counterparts (Galen et al. 2000). NESARC’s survey of the noninstitutionalized population showed a stronger association between ASPD and substance use disorders in women than in men;however, this may be, in part, because men are overrepresented in criminal justice populations left out of the sample (Grant et al. 2004b). Assessment of possible ASPD in substance abuse treatment clients can be confounding.Many clients have exhibited antisocial behavior during their drug use that does not justify an ASPD diagnosis. People may display antisocial symptoms in one context, such as prison, but not another. Diagnosis for ASPD is generally based on the client’s history as well as his current behavior. Forrest (1994) describes some of the difficulties of and alternative approaches to differential diagnosis in his book, Chemical Dependency and Antisocial Personality Disorder. Treatment of men with ASPD in substance abuse treatment settings can be difficult. In fact, certain elements of usual substance abuse treatment can make people with ASPD anxious and prone to act out in treatment. Often,substance abuse treatment emphasizes emotional sharing, personal disclosure, honesty,and confronting shame—all of which may feel provocative and overwhelming to men with ASPD. Clients who are antisocial may manipulate staff members and other clients, violate or flout program rules, be intentionally deceptive, shame or abuse others, attempt to control the treatment environment and, as a last resort, leave treatment early. As a result, people with ASPD may require special treatment that provides a safe and contained environment in which to manage their anxiety. In early treatment, counselors may need to emphasize controlling negative behavior and compliance with rules while downplaying emotional expression and interpersonal sharing, and they should establish clear consequences for violating program rules (though these might seem draconian in other treatment settings). Treatment programs for co-occurring ASPD and substance abuse are often found in prison settings, but many clients who could benefit from such programs are not in prison. A community alternative is the establishment of long-term residential therapeutic communities (TCs), although not all TCs are appropriate for people with ASPD. SuicidalityA variety of mental and substance use disorders can increase a man’s risk for committing suicide; therefore, although it is not a disorder per se, suicidality must be addressed. Women are three times more likely to attempt suicide than men, but men are more than four times as likely to die from suicide (NIMH 2001). Infact, researchers have found this to be true across cultures, with a few notable exceptions,such as mainland China (Arsenault-Lapierreet al. 2004). The highest rate of completed suicide among any demographic group occurs inWhite American men ages 65 and older (U.S.Public Health Service 1999). Higher rates of suicide completion among men may result, in part, from the deadlier methods men typically choose for suicide. For example, 79 percent of all suicides using fire arms are committed by White men, and fire arms are involved in most(58 percent) completed suicides (Antai-Otong2003). Additionally, men tend to perform fewer suicidal acts but exhibit a higher intent to die (Nock and Kessler 2006).
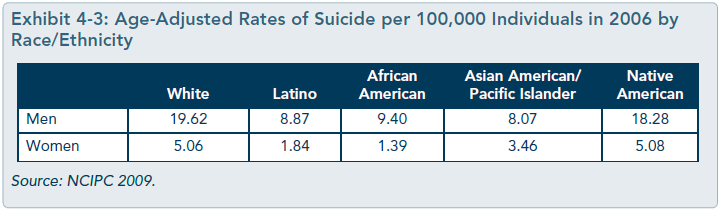
Substance use and abuse are major risk factors for suicide; men with substance use disorders have high rates of death by suicide (Wilcox etal. 2004). Approximately 30 to 40 percent of suicide attempts and completed suicides involve acute alcohol intoxication (Cherpitel etal. 2004). Substance-related problems appear to be more often associated with suicide in men than in women, suggesting an even greater need to screen for suicidality among men intreatment (Arsenault-Lapierre et al. 2004). [Question #66. Substance use and abuse are major risk factors for:] Co-occurring mental disorders increase the likelihood of suicide even more than substance abuse alone: depression, schizophrenia, bipolar disorder, and personality disorders all increase the chances that someone will both attempt and complete suicide (Arsenault-Lapierre etal. 2004; Blumenthal 1988). Other factors,such as certain physical ailments (e.g., epilepsy,cancer, Huntington’s chorea) and a family history of suicide, also appear to increase the likelihood of suicide (Blumenthal 1988). Rates of death by suicide vary by race and ethnicity. Exhibit 4-3 depicts age-adjusted rates of suicide per 100,000 individuals in the year 2006 according to the Centers for Disease Control and Prevention’s (CDC’s) National Center for Injury Prevention and Control(NCIPC; 2009). Appendix D of TIP 42 (CSAT 2005c) recommends that all substance abuse treatment clients receive at least a basic screening for suicidality and notes a particularly high risk among clients who have relapsed to substance use after an extended period of abstinence.TIP 42 (Chapter 8 and Appendix D) also listskey questions for evaluating suicide risk and provides other information on this topic. TIP 50, Addressing Suicidal Thoughts and Behaviors in Substance Abuse Treatment (CSAT 2009a), provides more data on suicide by men and women with substance use disorders as well as information on and case studies relating to addressing this issue in substance abuse treatment.TIP 50 proposes that counselors use a four-step screening and intervention process with clients who may be suicidal: (1) Gather information, (2) Access supervision, (3) Take responsible action, and (4) Extend the action.These steps, known by the acronym GATE, are described in the text box on the next page. [Question #67. The steps for GATE process with clients who may be suicidal are:] Men With Physical Health ProblemsMen with substance use disorders are at increased risk for a wide range of medical conditions either caused or exacerbated by their substance use, including various cancers, cardiovascular and pulmonary conditions, neurological problems, gastrointestinal disorders,endocrine syndromes, and hepatic disorders (Mannelli and Pae 2007; Ries et al. 2009;Saitz 2009). They are also at increased risk for infectious diseases, including viral hepatitis (see TIP 53, Addressing Viral Hepatitis in People With Substance Use Disorders [SAMHSA 2011a]) and HIV/AIDS (see the “Men With HIV/AIDS” section on p. 84 of this TIP; see also TIP 37, Substance Abuse Treatment for Persons With HIV/AIDS [CSAT 2000c]). Some such illnesses (e.g., liver cirrhosis) may result directly from the substances used, whereas others (e.g., HIV/AIDS) may result from the method of drug administration or the lifestyle that accompanies substance abuse. [Question #68. Diseases resulting from the method of drug administration or the lifestyle that accompanies substance abuse is: ]
 An Overview of GATEG: Gather information. There are two steps to gathering information: (1) screening and spotting warning signs and (2) asking follow-up questions. Screening consists of asking brief, uniform questions at intake to determine if further questions about suicide risk are necessary. Spotting warning signs consists of identifying telltale signs of potential risk. Counselors should ask follow-up questions when clients respond “yes” to one or more screening questions or whenever they notice a warning sign. Asking follow-up questions elicits as much information as possible so that counselors and their supervisors and/or treatment teams can develop a good plan of action. Counselors should provide as much information as possible to other providers upon referring their clients to them.
A: Access supervision and/or consultation. Counselors should never attempt to manage suicide risk alone in clients, even if they have substantial specialized training and education. With suicidal clients, two or three heads are almost always better than one. Therefore, counselors should speak with a supervisor, an experienced consultant who has been vetted by their agency, and/or their multidisciplinary treatment team when working with a suicidal client. It is a collective responsibility, not the counselor’s alone, to formulate a preliminary impression of the seriousness of risk and to determine the action(s) that will be taken. Accessing supervision or consultation provides invaluable input that promotes the client’s safety, gives counselors needed support, and reduces personal liability. T: Take responsible action(s). A counselor’s action(s) should be responsible and make good sense in light of the seriousness of a client’s suicide risk. Some of the potential actions (which cover a range of intensity and immediacy) that counselors and their supervisors or teams may take include:
Upon a return to acute suicidality, create a safety card with the client. TIP 50 (CSAT 2009a, p. 21), describes this process.
E: Extend the action(s). Too often, suicide risk is dealt with once, in acute fashion, and then forgotten. As with substance abuse, vulnerable clients may relapse into suicidality. Thus, counselors need to continue to observe and check in with clients to identify any possible return of risk. Another common problem is referring a suicidal client but failing to coordinate or follow up with the provider. Suicide risk management requires a team approach, and a client’s substance abuse counselor is an essential part of this team. A counselor should document all actions taken to create a medical and legal account of the client’s care: what information was obtained, what actions were taken and when, and how follow-up on the client’s substance abuse treatment and suicidal thoughts and behaviors was conducted. This record can be useful for supervisors, consultants, the counselor’s t eam, and other providers. Source: CSAT 2009a, pp. 14–15. Adapted from material in the public domain. The consensus panel recommends that all clients entering substance abuse treatment programs have a thorough physical examination with appropriate laboratory studies. Programs should also provide medical services or link to such services; doing so can improve recovery outcomes for clients (Friedmann et al. 2003,2009). Integrated medical care results in better abstinence outcomes than independent but linked services (Weisner et al. 2001), and onsite services result in better use of medical care than offsite services (Friedmann et al. 2001). Men With HIV/AIDSThe HIV/AIDS epidemic is not uniform in distribution; prevalence varies considerably across the country, not only from region to region, but also within regions, States, and even communities. However, men have consistently been more affected by HIV/AIDs than women. CDC’s HIV/AIDS Surveillance Report estimates that, in 2007, men ages 13 and older made up 74 percent of current HIV/AIDs cases and 73 percent of cases diagnosed in thatyear (CDC 2009). Between 2003 and 2006,the number of HIV/AIDS cases increased approximately 5 percent for men but decreased 6 percent for women.
Encouraging men at risk for HIV/AIDS infection to obtain counseling and testing is a priority. In men, HIV/AIDS is most often transmitted by men having sex with othermen, but injection drug use is the second most common transmission method among men (CDC 2009). Men who have sex with men may also engage in substance abuse and are more likely to have unprotected sex if under the influence (Purcell et al. 2001). About 17 percent of men ages 13 and older who had HIV/AIDS in 2006 may have acquired the disease by injecting drugs (CDC 2008b). Men with HIV/AIDS can have great difficulty accessing services. The added complication of a substance use disorder can create even more troublesome barriers to seeking treatment. Societal attitudes toward men with HIV/AIDS in particular areas of the country,such as certain rural communities, can contribute to even larger gaps in service for this population (Heckman et al. 1998; Shernoff1996). For more information on HIV/AIDS and substance abuse treatment for men who are HIV positive, see TIP 37 (CSAT 2000c). Stigma can make men reticent about discussing their HIV/AIDS status with counselors.Clinicians who know that a client is HIV positive should speak privately with him about whether he wishes to identify as such to other group members. Counselors should caution clients of the possible negative effects of disclosure even in a treatment setting and help them carefully consider pros and cons. Men With Physical DisabilitiesMen with disabilities may experience more prejudice than other men because their disabilities keep them from meeting cultural expectations about male bodies and behavior.This causes gender role stress and makes it difficult for some men with disabilities to fulfill certain socially defined gender roles. Men are socialized from an early age to be active,independent, tough, self-confident, athletic,and self-reliant—but having a disability can limit a man’s ability to satisfy some or all of these roles (Marini 2001). Society typically views people with disabilities as helpless, incapable, and inferior (Lyons 1991). Ironically, for many men with severe disabilities, their substance use, even though problematic, may represent one of the last masculine behaviors remaining available to them. TIP 29, Substance Use Disorder Treatment for People With Physical and Cognitive Disabilities (CSAT 1998e), provides information on substance abuse treatment for people with physical disabilities.
Traumatic Brain InjuryMen are at higher risk for violence in our society, and therefore, they are also at higher risk for traumatic brain injury (TBI). TBI results from a sudden blow to the skull due to collision (causing a concussion), sudden penetration of the skull, blast pressure waves, or the head being thrust out of position. The injury may damage a specific part of the brain or diffuse throughout the brain tissue. TBI symptoms can be subtle and thus go unrecognized in many people; moreover, the symptoms are often similar to those caused by other problems, resulting in misdiagnosis. TBI symptoms may last only a few days or weeks, or they may be permanent. Even mild TBI can produce long-lasting cognitive and behavioral effects that significantly impair substance abuse recovery. For instance, a person’s ability to accept and integrate information in treatment may be compromised by TBI. The injury may also cause the person to act impulsively without being able to explain why. TBI symptoms can include:
Treatment should be adapted to meet the specific needs of clients with TBI:
These resources provide more information on recognizing and treating clients with TBI:
Source: CSAT, 2010b. Adapted from material in the public domain. Men From Different Age GroupsYoung men often feel great pressure to show their masculinity. As men grow older, their beliefs about masculinity and the social expectations for masculine behavior change. Similarly, men’s substance use/abuse often changes over the course of their lives. Age, therefore,can be a significant factor in determining substance abuse patterns and appropriate treatment for substance abuse.
Specific Needs of Younger Men Entering TreatmentYoung adult men, typically defined as men ages 18 to 24 (Park et al. 2006), have issues related to masculinity and substance abuse that distinguish them from men in other age groups. Drug and tobacco use, binge drinking,and recent illicit drug use are most common in this age group and are more common for men in this age group than for women (Park et al.2006). In this age group, men are three times more likely than women to die, and high rates of death by automobile crashes, homicide, and suicide account for much of the difference (Park et al. 2006; Pollack 2010). Among young men in certain cultural/ethnic groups (notably Native American and African American men),rates of violent death are considerably higher.Frequent or binge alcohol use and frequent drug use have been associated, in diverse samples of young men, with increased risk for being the victims of violence; these behaviors appear to increase young men’s likelihood of being perpetrators of violence as well (Cooperet al. 2000; Friedman et al. 1996; Richardsonand Budd 2003). For both younger and older adults, binge drinking has been associated with significant alcohol-related problems, and men (15 percent) are more likely than women (4.7 percent) to binge drink (Blazer and Wo 2009a). In one study, younger men were five times as likely to be involved in fighting or violent crime and seven times as likely to break or damage something as their counterparts who drank less frequently and did not binge drink (Richardson and Budd 2003).
High rates of substance use/abuse and violence may reflect the fact that young men are often less secure about their masculinity than older men and therefore may feel a greater need to engage in behaviors that supposedly prove their masculinity to others. Take, for example, the elevated death rate by automobile collision among men in this age group. This results largely from the fact that young men are the least likely of men in any age group to use seat belts and the most likely of men in any age group to be in a crash in which at least one driver is alcohol impaired (Park et al. 2006).Young men also engage in a variety of other high risk behaviors. For example, young men who inject drugs are more likely to engage in practices that put them at high risk for contracting HIV (Rondinelli et al. 2009). [Question #70. High rates of substance use/abuse and violence in the young male population reflect:] Heavy drinking and illicit drug use can be seen as high risk behaviors that young men engage in, in part, to demonstrate their masculinity. Research by Peralta (2007) found that most undergraduate students (both male and female) agreed that drinking was generally perceived as an activity that expressed masculinity. More White American (76 percent) than African American (53 percent) students held this belief, suggesting that cultural background influences attitudes about masculinity and drinking. Students interviewed for the study spoke of the beliefs that being able to hold your liquor was a sign of masculinity and that bouts of heavy drinking were rites of passage for men (but not women). Other types of substance use may also be perceived, in certain cultural contexts, as ways of expressing masculinity. Brown (2010) evaluated methamphetamine use among young Native American and White American men in Appalachia and found that use of the drug was linked with a strong masculine identity, but admitting that one had a problem with the drug (e.g., by entering treatment) was considered a sign of weakness. In other contexts, success in the drug trade is also considered an expression of a strong masculine identity (Bourgois 2003). Young men may have some unique substance abuse treatment needs, although these vary according to cultural and sociodemographic factors. For example, young men who have made a living from the drug trade or other criminal activity may need vocational training and help finding a job, whereas college students in recovery value alcohol-free housing (i.e.,dorms) and social activities (Bell et al. 2009). Young men often enter treatment under coercion (by family, the criminal justice system,schools, and/or employers), and thus more effort may be needed to help them move from an early stage of readiness for change (precontemplation) toward embracing and accepting abstinence. The largest single source of treatment referrals for individuals (both male and female) in this age group is the criminal justice system, which accounted for 52 percent of first-time admissions and 46 percent of return admissions in 2006; the percentages for men alone are likely higher (SAMHSA, OAS2008a). In comparing young adults to those ages 26 to 45 in a largely (85 percent) male,probation-referred treatment population,Sinha and colleagues (2003) found that young adults were significantly more likely to be in precontemplation but significantly less likely to be in contemplation, determination, or maintenance stages than adults ages 26 to 45.Young adult male clients may also be more resistant to involvement in mutual-help groups, especially when groups specifically for younger people are unavailable. Transference-related issues can arise for younger clients who have older counselors. Some transference may be positive and useful for treatment, but much may be negative, causing clients to rebel against the advice and support of older counselors. [Question #71.The largest single source of substance abuse treatment referrals for individuals in younger age groups is the criminal justice system. True/False? ] Data on substance abuse treatment programs specifically geared toward young adult men are limited, but various program models have been tried with this population (including gender-specific programming), particularly in criminal justice settings. Research into TCs (see Chapter 5) shows that young adult men are less likely than other clients to be involved with or integrated into the TC (Chan et al. 2004),perhaps because they have a greater need to rebel against the high degree of structure offered by TCs. Even so, this should not disqualify the TC approach, which has been found useful for young men (more so than older men) in prison settings (Messina et al. 2006). Data suggest that adults who begin using substances at a younger age are more likely to be classified as substance dependent when they get older than those who start using substances later in life. Some boys start using alcohol or tobacco in the fifth or sixth grade or even earlier (SAMHSA 2005; Vega et al. 1993).Boys may start to use substances at an especially early age because of factors in their school environments, such as availability of drugs on or near the school campus (National Institute on Drug Abuse 1999), or because of substance abuse in their homes. Specific Needs of Older Men Entering TreatmentMen 55 years of age and older often decrease or end their alcohol and drug use, and their rates of substance use disorders decline as well. A number of factors contribute to these changes, including early mortality among individuals who drink heavily and/or use illicit drugs, negative effects of substances on medical problems, additional medical problems caused by substance use, decreased desire to use, potential financial strain, and less participation in social events and activities focused on substance use (Menninger 2002). However,other factors, such as loneliness and depression, may cause some older adults to increase their drinking (Capraro 2000; Strowig 2000).Some of these factors may affect men and women differently. For example, older men seem less concerned than older women about the effects of alcohol on their health (Satreand Knight 2001), which may help explain why older age is associated with greater decreases in alcohol consumption for women than for men (Satre and Aren 2005).
In SAMHSA’s 2007 National Survey of Drug Use and Health (NSDUH), a survey of the general U.S. population ages 12 and older, 2.6 percent of men ages 65 and older met criteria for a past-year alcohol use disorder (U.S.Department of Health and Human Services [HHS], SAMHSA, OAS 2008a). Other studies have found higher rates (see review in Satre and Aren 2005). Also in the 2007 NSDUH,a greater percentage of men than of women over the age of 65 reported drinking more than the amount recommended by the National Institute on Alcohol Abuse and Alcoholism (NIAAA), which is no more than one drink per day for older men (NIAAA 2005). Among those ages 65 and older who reported drinking at least one drink in the prior month, 48.7 percent of men reported more than one drink per day compared with 28.7 percent of women; 17.7 percent of men reported more than two drinks per day (HHS, SAMHSA, OAS 2008a). Although rates of alcohol abuse/dependence declined with age for both men and women, the extent of that decline was greater for women than for men.In the 2007 NSDUH, men ages 65 and older were 37.5 times more likely to not have a past-year alcohol problem than to have one; women in the same age group were 249 times more likely (HHS, SAMHSA, OAS 2008a). Data from SAMHSA’s 2005 and 2006 NSDUH surveys (Blazer and Wu 2009a)show that men ages 65 and older were more likely to engage in binge drinking if they had higher incomes; were separated, widowed, or divorced; smoked; and/or used illicit drugs. As with younger men, men ages 65 and older were significantly more likely to binge drink (14 percent) than were women (3 percent).Research with older adults who have completed treatment also shows that older men have greater difficulty than older women maintaining abstinence after substance abuse treatment(Satre et al. 2004a; Satre et al. 2004b). Although published data on the abuse of substances other than alcohol by adults older than 55 is limited, many researchers have raised concern about the misuse and abuse of preblockedion drugs by this population (Blazer and Wu 2009b; Simoni-Wastila and Yang 2006).Some studies describe preblockedion drug abuse as less common among older men than older women (Simoni-Wastila and Yang 2006); others conclude the inverse specifically for pain medication (Blazer and Wu 2009b). For more information, see SAMHSA’s Get Connected! Linking Older Adults With Medication, Alcohol,and Mental Health Resources toolkit (2003). Also see TIP 26, Substance Abuse Among Older Adults (CSAT 1998d), which recommends that substance abuse treatment programs for both male and female older adults:
Gay and Bisexual MenGay and bisexual men generally have higher rates of substance use and substance use disorders than heterosexual men, although some research indicates that the rates are becoming more similar between these groups (Cochranet al. 2000). NESARC data showed that men who self-identified as gay were 4.4 times as likely as heterosexual men to have used marijuana in the past year, 3.5 times as likely tohave used other drugs, 2.9 times as likely to have past-year alcohol dependence, and 4.2times as likely to have past-year dependence on a drug other than marijuana (McCabe et al.2009). Odds ratios for bisexual men, compared with heterosexual men, were even greater.Cochran and colleagues (2006) found that men with male partners were significantly more likely than men with female partners to report lifetime illicit drug use (72.8 percent and 54.6 percent, respectively) and were 2.4 times as likely to meet criteria for problematic drug use.
Gay and bisexual men entering substance abuse treatment, compared with heterosexual men, report more frequent use of their primary substance of abuse and are more likely to primarily abuse methamphetamine, to have had prior hospitalization for mental health issues, to be homeless, and to report being victims of domestic abuse; they are less likely to primarily abuse alcohol or marijuana or to have current legal problems (Cochran and Cauce 2006). However, gay and bisexual men are significantly more likely than heterosexual men to seek treatment for substance use and/or mental disorders (Grella et al. 2009a). Much of the disparity in alcohol and drug consumption rates between gay/bisexual and heterosexual men may be connected to the fact that, within gay culture, clubs, bars, and parties at which alcohol and drugs are consumed continue to be important and widely used social outlets (CSAT 2001; Weidel et al. 2008). A Provider’s Introduction to Substance Abuse Treatment for Lesbian, Gay, Bisexual, and Transgender Individuals (CSAT 2001) provides more information on substance abuse treatment for gay and bisexual men. It recommends that clinicians be sensitive to gay cultural norms, prejudices against gay men,and social expectations related to gay culture that may affect substance use. The sexual orientation of both client and counselor can complicate the issue of gender bias in the therapeutic relationship. For example, a gay male substance abuse client may expect that a straight male counselor, due to his own socialization and bias, will be judgmental and potentially shaming. As a result, gay men in substance abuse treatment settings may be more cautious about coming out and discussing issues related to relational/social aspects of their substance abuse experiences or their primary relationships. As with gender considerations, the sexual orientation of the client and counselor should be considered when assigning counselors to substance abuse treatment clients. Gay male clients may feel more comfortable working with a woman or a gay male counselor. If a gay client is matched with a gay counselor, the issue of sexualized transference will most likely need to be addressed. It is not always possible to match clients and counselors with regard to sexual orientation, so counselors need to explore and challenge their own sexual orientation biases and beliefs to work effectively with gay men in substance abuse treatment settings. [Question #72.Counselors need to explore and challenge their own sexual orientation biases and beliefs to work effectively with gay men in substance abuse treatment settings. True/ False?] Men With Employment or Career-Related IssuesEmployment-related issues (e.g., type of job,lack of employment) can strongly affect men’s substance use/abuse, and men with substance use disorders are at greater risk for unemployment.The link between SES and substance abuse is more complex (see text box below).
For men who are employed, their type of profession may affect the pattern and extent of their substance use. For example, research has shown a relationship between drinking and having positions that are typically male dominated. Men who work in “precision production, craft, and repair jobs, and those who [a]re operators, fabricators, and laborers” have higher rates of alcohol use and dependence (OAS2002, p. 3), and those in physically risky positions (e.g., maintaining heavy machinery, operating light machinery, working with hazardous chemicals) are more likely to use substances than those in less risky positions (Lehman and Bennett 2002). In some professions, use of certain substances (usually alcohol) is considered normal behavior and not using is seen as anomalous among men. In treatment, this can be an issue for men who must decide whether to return to a job or type of employment that may, in some ways, promote drinking or drug use. It may be difficult for a man to return to such a work setting, but it can be equally as difficult for him to leave a career that has helped define who he is. Counselors may find it useful to discuss work-related concerns with clients and to use role-playing and other methods to help them develop strategies for avoiding substance use at work or in other settings where they may feel pressure to use. Whether a client has a job or not, employment and work-related issues should be addressed in treatment. Ask male clients about positive and negative aspects of work in their lives and talk with them about their work-related goals. Doing so may help them see how substance abuse has affected their work and how recovery can positively influence their careers and offer other means for fulfillment (Lyme et al. 2008). Some men with jobs do not have insurance or sick leave to use for treatment, or they are unwilling to seek treatment for fear of risking their employment. In SAMHSA’s 2007 NSDUH, men who needed substance abuse treatment were more than 16 times as likely as women who needed treatment to express concern that entering treatment would affect their jobs (HHS, SAMHSA, OAS 2008a). Socioeconomic Status and Men’s Substance AbuseResearch on men’s economic class and its relation to substance abuse usually focuses on men with lower SES. This may be because men of lower SES are overrepresented in substance abuse treatment populations, particularly those receiving public funds. However, data supporting the claim that men of lower SES are more likely to abuse substances are inconsistent at best. The relationship of substance use and abuse to SES appears to depend, in part, on the type of substance involved. For example, surveys consistently show that men living below the poverty line are more likely to smoke cigarettes than those with higher incomes (CDC 2004), and research has associated past-year marijuana use with lower incomes and unemployment (Robertson and Donnermeyer 1998). People of lower SES are also more likely to have drinking-related problems (Crum 2003) despite greater consumption of alcohol being associated with higher socioeconomic status (Casswell et al. 2003; van Oers et al. 1999). SES apparently interacts with other factors (e.g., age, gender, acculturation) to influence alcohol consumption. Changes in income or status may also affect substance use and abuse; men who unexpectedly or unwillingly move from a higher to a lower SES can experience anxiety and depression, which are associated with substance use and abuse (Hemmingsson et al. 1999; Timms 1998).
[Question #73. Employment-related issues that can strongly affect men’s substance use/abuse are:] Men Who Are UnemployedMen without jobs have a surplus of time—and sometimes, too few constructive activities with which to fill it. Men, who are traditionally expected to be the bread winners in American society, often experience lowered self-esteem as a result of unemployment, which can lead to despair and hopelessness. Men who have lost a job often increase their alcohol consumption (Dooley and Prause 1998). When a man loses his job, is demoted, or loses social status in some other way, the resulting anxiety may lead him to use problematic coping techniques, such as substance use (Liu 2002).
Men who are unemployed are more likely to be currently using a substance than those with full-time jobs, and people with substance use disorders are more likely to be unemployed than the general population (Platt 1995). According to 2003 data, 18.2 percent of unemployed adults were currently using illicit drugs compared with 10.7 percent of those employed part time and 7.9 percent of those employed full time. Current alcohol use was slightly greater among people with jobs, but heavy use (five or more drinks on five or more occasions in the past month) was greater among those without jobs (OAS 2004b). Men entering substance abuse treatment are more likely to be unemployed than employed.Data from 2006 showed that 68 percent of men admitted to substance abuse treatment programs that received State agency funds were unemployed or not in the labor force (HHS, SAMHSA, OAS 2008a). Unlike men with jobs, who are sometimes willing to seek substance abuse treatment to keep their positions, men who are unemployed may lack important help-seeking resources like employee assistance programs and health insurance. Employment has been correlated with successful treatment outcomes (Platt 1995). A study by Arndt and colleagues (2004) found a positive association between abstinence and full-time employment for men after treatment.For more information on the relationship between employment and treatment success, as well as integrating vocational training into substance abuse treatment programs, see TIP 38, Integrating Substance Abuse Treatment and Vocational Services (CSAT 2000a). Men Who Are VeteransIn 2006, veterans accounted for over 66,000 admissions (4.9 percent of total admissions) to substance abuse treatment programs tracked by SAMHSA’s Treatment Episode Data Set(TEDS); most (91.4 percent) were men. The most common source of referral for male veterans, as it is with all men, is the criminal justice system, accounting for 36.7 percent of admissions (HHS, SAMHSA, OAS 2008a).
Estimated rates of substance abuse are similar for veterans and non veterans, but male veterans receiving treatment are more likely than male non veterans to report alcohol as the primary substance of abuse (59 percent and 40.4 percent, respectively; HHS, SAMHSA, OAS2008a). Veterans treated in VA facilities (see advice box on the next page) have significantly more problems than patients in non-VA facilities with employment, education, legal issues,and co-occurring mental and medical disorders (Veterans Health Administration 1996).Furthermore, VA programs serve a large number of veterans who are homeless, many of whom have co-occurring substance abuse and mental disorders (Kasprow et al. 1999). About 50 percent of VA substance abuse treatment program clients also have one or more co-occurring mental disorders (Tracy et al. 2004). An analysis of data from the National Survey of Homeless Assistance Providers and Clients found that, for clients who are homeless, being male increased the odds of having an alcohol problem by nearly 3 times, whereas being a veteran increased the odds by 1.3 times (Dietz2007). Being male and/or a veteran similarly affected the odds of having a drug problem. Advice to Behavioral Health Clinicians: Accessing VA ServicesTo be eligible for treatment in the VA system, veterans must have served in the U.S. Armed Forces and received an honorable military discharge or general discharge under honorable conditions, subject to minimum duty requirements. VA substance abuse treatment facilities provide inpatient, residential, and outpatient services. A variety of VA programs exist to help veterans who are homeless obtain health care, vocational rehabilitation, job training, and transitional or permanent housing.
Veterans can be referred to VA services by any treatment provider and can register for services via the member services office at their local VA facility. They must bring a copy of their discharge papers and may be charged a copay if their annual gross income exceeds a given amount (exceptions being any veteran who served in Vietnam or has a service-connected disability). To reach veterans in rural or remote areas, the VA has community-based outpatient clinics linked to major VA medical centers. For more information on how to access VA services, find local VA resources, and so forth, visit VA’s “New to VA” Web site (http://www1.va.gov/opa/newtova.asp). Real Warriors also offers numerous resources for veterans (http://www.realwarriors.net/veterans/treatment/substanceabuse.php; 1-866966-1020), including opportunities to speak over the phone or chat live on the Web with a trained health resource consultant at the Defense Centers of Excellence Outreach Center. Men With Systems-Related NeedsMen enter treatment with multiple needs, as their substance abuse has likely affected every aspect of their lives. Often, a man’s behavior involves him with a system (e.g., the criminal justice system) that may require his treatment providers to interact with that system. In othercases, other systems may be required to provide for a man’s specific needs (e.g., housing).Some such systems (medical services, VA services, and vocational rehabilitation) have already been covered in this TIP; two more that involve many men in treatment (housing and homelessness services and the criminal justice system) are discussed in the following sections.
Men Who Are HomelessIt is difficult to ascertain the total number of men who are homeless in the United States;nevertheless, the National Survey of Homeless Assistance Providers and Clients (the largest survey of its kind) found that 61 percent of adults who were homeless and sought services in 1999 were men living alone. Another 24 percent were men living with another person.Of men in the survey who were homeless, 33 percent were veterans (Burt et al. 1999).
Men also make up a large percentage of adults who are homeless and seek treatment for substance abuse. In SAMHSA’s 2006 TEDS study, men comprised 75.6 percent of individuals who were homeless and entered substance abuse treatment programs that received funding through State agencies (HHS, SAMHSA,OAS 2008b). Substance use disorders are especially common among men who are chronically homeless; according to one study, they occur in 84 percent of men compared with 58 percent of women (North et al. 2004). Burt and colleagues’ (1999) review of data from programs that provide homelessness services found that 73 percent of clients were male.Out of the total client population, 66 percent reported at least one alcohol, drug, or mental problem in the month prior to their interview,74 percent reported such a problem in the past year, and 86 percent reported a problem at some time during their lives. Alcohol was the most commonly abused substance; 38 percent of clients reported alcohol problems in the past month, 46 percent reported such problems in the past year, and 62 percent reported problems with alcohol during their lifetime. In terms of other substances of abuse, 26 percent of clients reported a drug problem during the past month, 38 percent during the past year,and 58 percent during their lifetimes. In a large survey, 46 percent of men who were homeless reported alcohol problems, whereas only 22 percent of women who were homeless did; men were also 50 percent more likely to report a problem related to illicit drugs (Burtet al. 1999). Men who are homeless are more likely than other men to have various concurrent problems ranging from high levels of shame and low self-esteem to HIV/AIDS and co-occurring disorders. A number of specific treatment interventions are considered promising for clients who are homeless, including modified TCs, intensive outpatient programs, contingency management approaches, motivational enhancement techniques (e.g., motivational interviewing),the provision of transitional and supportive housing for individuals who were formerly homeless, and intensive case management(Begun 2004; Zerger 2002). Treatment retention is a particular problem for providers working with men who are homeless (see advice box below). For more on substance abuse treatment for clients who are homeless, see TIP 55, Behavioral Health Services for People Who Are Homeless (SAMHSA 2013). [Question #74. Treatment retention is a particular problem for providers working with men who are homeless. True/ False?] Researchers have noted the potential benefits of gender-specific treatment for women who are homeless and have substance use disorders (Zerger 2002). However, despite the fact that men who are homeless outnumber women who are homeless in treatment 4 to 1, little research has been done to determine the best interventions for this specific population.Kraybill and Zerger (2003) reviewed six substance abuse treatment programs for clients who are homeless that they recognized as providing effective services; one of these, CasaLos Arboles (a component program of Albuquerque Health Care for the Homeless),provides services specifically to men. This 6 to 9-month intensive inpatient program uses staff members recovering from substance abuse, intensive case management, and a slow process of transition to independent living for clients. In the orientation phase, which lasts 45days, clients cannot leave the premises on their own—this and other privileges are introduced slowly. Overall, the program is much more rule-bound than the equivalent program for women at Albuquerque Health Care for the Homeless. [Question #75. Casa Los Arboles, an intensive inpatient program that provides services specifically for homeless men, use staff members recovering from substance abuse. True/ False?] Advice to Behavioral Health Clinicians: Increasing Retention Among Clients Who Are HomelessTraditional substance abuse treatment models are often ineffective for individuals who are homeless. Dropout rates of two thirds or more are seen in this population; thus, engagement and retention are areas that any program working with men who are homeless must address.
Based on the experiences of eight NIAAA grantees providing treatment to men and women who were homeless (six of which served a primarily male client base), Orwin and colleagues (2001) suggested the following ways to increase retention:
Men Involved in the Criminal Justice SystemMen who require treatment for substance use disorders may hesitate to seek services out of fear that acknowledging and seeking help for problems with substances may complicate their legal difficulties; they may fear that their insurance providers will consequently refuse to pay for treatment or that they will be turned over to legal authorities. Other men may be reluctant to acknowledge a history of arrest and incarceration and may fear that this information will be revealed if they enroll in a treatment program. Thus, many men may resist needed care. Behavioral health counselors should not offer legal advice, but they can help clients recognize when to seek professional legal counsel and can refer them appropriately.
Men are more likely than women to be involved in the criminal justice system, and this is reflected in referrals to substance abuse treatment from this system. In 2006, referrals from the criminal justice system accounted for 41.7 percent of all men entering substance abuse treatment programs that received public funds (compared with 30 percent of all women entering treatment), making it the largest single source of referral for men entering substance abuse treatment (HHS, SAMHSA, OAS 2008a). In addition to the many substance abuse treatment programs available for men who are incarcerated, 28 percent of all programs in 2006 offered services for criminal justice clients other than those convicted of driving under the influence (SAMHSA, OAS2007a). TIP 44, Substance Abuse Treatment for Adults in the Criminal Justice System (CSAT 2005b), provides more information on treatment options available for men in the criminal justice system. TIP 30, Continuity of Offender Treatment for Substance Use Disorders From Institution to Community (CSAT 1998b), offers information on working with clients who are making the transition from criminal justice institutions to the community. Men involved in the criminal justice system may be affected differently than women by certain factors. For example, a large study of men and women treated in prison-based TCs found that men who were employed prior to incarceration were significantly less likely to return to custody in the 2 years after treatment than those who were unemployed, which was not the case for women (Messina et al. 2006).However, men who were employed were also less likely to enter continuing care, suggesting that although having a history of employment helped men avoid returning to custody (possibly because it enabled further employment),employment may have also made them less interested in or less able to participate in further treatment following incarceration. Men in correctional settings and men on probation or parole often have unique needs in substance abuse treatment. For instance, men in prison may have different ways of thinking about and judging specific behaviors than men on the outside. These cognitive distortions are not necessarily distortions in the context of prison life, but rather are useful for managing day-to-day prison life. Criminogenic patterns can influence a man’s values, beliefs, attitudes,and emotion management; therefore, the patterns need to be identified and addressed in treatment. Adaptations that can help a man survive in prison may be maladaptive in the community or in substance abuse treatment program settings. Persons entering substance abuse treatment after incarceration may benefit from training to build skills for coping and operating successfully in the free world.Treatment for men who have been imprisoned should also address recidivism and relapse. Men currently involved with the criminal justice system as well as those who leave it to enter substance abuse treatment may be reluctant to divulge information, resistant to expressing vulnerable emotions (e.g., sadness, fear), or hesitant to interact in group treatment. Behavioral health counselors should try not to interpret these behaviors as resistance, denial,uncooperativeness, or unwillingness to participate in recovery. To do so may actually increase the negative, protective behavior. Serious, pervasive mental illnesses occur more often among men who have been incarcerated than those who have not (Center for Mental Health Services National GAINS Center for Systemic Change for Justice-Involved Persons with Mental Illness 2007). Men with mental illnesses are further traumatized in prison, and although their resulting adaptations may help them survive there, they can also make substance abuse treatment even more difficult. The GAINS Center offers specific suggestions and treatment options for people from the criminal justice system who have concurrent mental illness and a substance use disorder; for more information, visit the Center’s Web site (http://gains.prainc.com/). Men From Diverse Cultural and Geographic GroupsRates and patterns of substance use/abuse vary among men according to cultural group. Researchers generally investigate cultural differences using broad racial/ethnic categories;those categories are thus used here. However,each broad category encapsulates a diverse set of cultures, and intragroup differences may be greater than intergroup differences in many cases. Behavioral health service providers are encouraged to investigate the specific cultures of their clients and discuss those cultures with their clients.
SAMHSA’s NSDUH showed that among men in 2007, American Indians/Alaska Natives had the highest rates of past-year substance use disorders (17.6 percent) of any single group, and Asians had the lowest rates (7 percent). The same survey showed past-year rates of substance use disorders of 13.0 percent for non-Hispanic White men, 12.1 percent for African American men, and 12.2 percent for Hispanic/Latino men (HHS, SAMHSA,OAS 2008a). SAMHSA’s TEDS surveys individuals when they enter treatment and thus excludes the many men who need but do not receive treatment. Exhibit 4-4 presents data on substance preferences for men entering treatment by ethnic or racial group. Percentages are derived from State and jurisdiction reports of treatment admissions to programs that received public funds (directly or indirectly) in the year2005. With the exception of alcohol plus another substance, only the primary substance of abuse is indicated (SAMHSA, OAS 2008b). These data indicate, to some extent, how culture affects patterns of substance use/abuse. 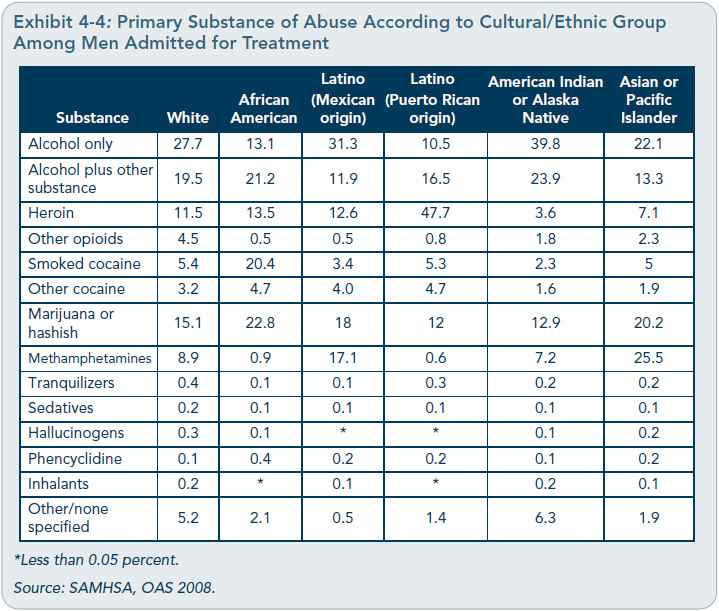 Information about substance use by diverse cultural groups of men is given in the following sections, as is information on specific substances and the populations that use them.Because of the gender rather than cultural focus of this TIP, this discussion of cultural issues is limited. More information can be found in the planned TIP, Improving Cultural Competence (SAMHSA planned c), which explores cultural and ethnic differences in substance abuse and discusses various culturally and ethnically based treatment issues.
African AmericansWithin-group diversityThe term African American is a broad denotation for an ethnocultural group of considerable diversity. The history and experience of African Americans has varied in different parts of the United States, and the experience of African American people in this country varies even more when considering the culture and history of more recent immigrants.
Today,African American culture embodies elements of Caribbean, Canadian, Latin American, European, and African cultures. Intragroup diversity among people of African descent is further influenced by numerous factors, including their country or region of origin; their upbringing; the extent to which their families conserve and perpetuate Afrocentric values,rituals, and beliefs; regional mores and customs; gender socialization; and age. The terms African American and Black are used synonymously at times, but some recent Black immigrants may not consider themselves African Americans, assuming that the term applies only to people of African descent born in the United States. African American men’s concept of masculinity may differ depending on their specific cultural background as well as their geographic location and SES, among other factors. For example, a study by Levant and colleagues (1998) found that African American men in the South endorsed significantly more traditional masculine roles than did African Americans from Northeast/Mid-Atlantic regions (the latter groups’ concept of masculinity more closely resembled that of White Americans). Admission/substance use statisticsAfrican American men made up 15.5 percent of all substance abuse treatment admissions to programs receiving funds through States in 2005 (SAMHSA, OAS 2008a). According to SAMHSA’s NSDUH, in 2006, the rate of past-month illicit drug use for African American men (ages 12 and older) was 13.8 percent;their past-year rate of heavy drinking was 13.4percent (HHS, SAMHSA, OAS 2007). Rates of crack cocaine use are higher for African American men than rates of methamphetamine, inhalant, or preblockedion drug abuse (HHS, SAMHSA, OAS 2008a).
Although young African American men are less likely to use drugs than young White American men, older African American men are more likely to do so—this is sometimes referred to as the crossover effect (French et al.2002; Watt 2008). A particularly powerful influence on increased drug use in this population is that African American men ages 35 and older are more likely to be offered drugs than are men in that age range from other racial/ethnic groups (Watt 2008). American Indians and Alaska NativesWithin-group diversityThe terms American Indian and Alaska Native refer to the indigenous peoples of North America, who collectively are often called Native Americans. There are 562 federally recognized American Indian and Alaska Native Tribes (SAMHSA, planned a), but there are also numerous Tribes recognized only by States and still others unrecognized by any government entity. Each represents a distinct culture; although similarities exist among certain Tribes, there are also significant differences.
More information on substance abuse treatment for this population is presented in the planned TIP, Behavioral Health Services for American Indians and Alaska Natives (SAMHSA planned a). Admission/substance use statisticsAmerican Indians and Alaska Natives comprise about 1 percent of the population of the United States (McKinnon 2003). However, in 2000, they constituted approximately 1.4 percent of individuals in substance abuse treatment programs receiving funds through the States (SAMHSA, OAS 2008b). Substance use patterns vary significantly among Native American Tribes, but within specific Tribes, American Indian and Alaska Native men usually have significantly higher rates of substance use disorders than women from the same Tribe. Rates of injuries, suicide, and homicide are disproportionately high among American Indian men, who are significantly less likely than American Indian women to receive medical services (Rhoades 2003).
NSDUH data from 2007 show that American Indians/Alaska Natives report the heaviest use of alcohol, tobacco, and many illicit drugs of any racial group (SAMHSA 2008). Rates of use are especially high for American Indian and Alaska Native men (HHS, SAMHSA,OAS 2007). American Indian men as a group have higher rates of binge drinking than the general population, but they also have higher rates of abstaining completely from alcohol than the general population (May and Gossage 2001; OAS 2007b). Drinking starts at an earlier age among American Indian men than their female counterparts (17 years versus 18.1 years, respectively), and American Indian men as a group have a tendency to drink more frequently and in larger quantities than American Indian women (May and Gossage 2001). Asians, Hawaiian Natives, and Other Pacific IslandersWithin-group diversityAsian Americans comprise over 30 diverse ethnic groups (e.g., Chinese, Filipino, Asian Indian) who speak different languages, have different levels of acculturation, and may have different immigration statuses and levels of income. This complexity is increased by key variables, such as reasons for migration, degree of acculturation, English proficiency, family composition and intactness, education, and adherence to traditions or religious beliefs.
Although they come from distinct cultures,Native Hawaiians and other Pacific Islanders are often grouped together with Asian Americans in surveys and other research. They are a relatively small group; data from the U.S. Census 2000 show that 0.3 percent of the population reported some Native Hawaiian or other Pacific Islander ancestry (Grieco 2001), and accurate information concerning patterns of substance use and abuse is thus difficult to come by. Chang and Subramaniam (2008) discuss how Asian American cultural beliefs about appropriate masculine behavior influence such factors as male help-seeking and concepts of health. Admission/substance use statisticsAsian Americans generally use alcohol and illicit substances less frequently than other Americans, although there are variations among subgroups. Asian Americans rank lowest of all racial or ethnic groups in terms of past-year illicit drug use. According to 2007 data, Asian Americans ages 12 and older were also less likely than members of other racial groups to report current alcohol use (35.2 percent) or recent binge drinking (12.6 percent).Asian Americans had a relatively low rate (4.3 percent) of past-year alcohol use disorders in 2007 (SAMHSA 2008); in 2005, they comprised 1 percent of admissions to substance abuse treatment programs receiving State agency funds (SAMHSA, OAS 2008b). Among those who did enter treatment, methamphetamine and marijuana abuse rates were high.
Research suggests considerable variations in substance use/abuse patterns among men from diverse Asian American populations. For example, the National Latino and Asian American Study, the largest national study to assess substance use disorders among Asian Americans from diverse cultural backgrounds, found that Filipino American men were 2.38 times as likely to have a lifetime substance use disorder as Chinese American men (Takeuchi et al.2007). Other research indicates significant differences in substance use and abuse patterns according to specific Asian cultural group, as well as differences related to such factors as geographic location and acculturation. The use of alcohol and other substances is more common among Native Hawaiians than members of other ethnic and racial groups living in Hawaii. In an adult household survey of Hawaiian residents conducted in 1998, about 36.7 percent of Native Hawaiian men reported heavy drinking and 15 percent met diagnostic criteria for either alcohol abuse or dependence (Gatrell et al. 2000). White AmericansWithin-group diversityWhite Americans (also referred to as Caucasians), like other large cultural groups, are heterogeneous in historical, social, economic, and personal features, with many subgroups and subtleties. Many have been in the United States for three or more generations, but others are recent immigrants (Giordano and McGoldrick 2005). Many White Americans have European cultural roots, but growing numbers come from Middle Eastern or North African cultures. For many White Americans,such characteristics as gender, sexual orientation, socioeconomic status, geographic location, occupation, religion, and so forth may be more important than race in defining their sense of cultural identity.
Admission/substance use statisticsRecent data show that White Americans are the racial group most likely to report current(i.e., past-month) use of alcohol. Overall,White Americans report more illicit substance use and abuse than do most other major racial/ethnic groups, but rates of use and abuse of specific substances vary (SAMHSA 2008).White men made up 39 percent of all substance abuse treatment admissions in 2005,the largest subset in the treatment population(SAMHSA, OAS 2008b).
Alcohol seems to be the primary substance of abuse among White Americans, but differences in its use do exist among the sub populations in this community. For example,O’Dwyer (2001) reviewed a study that found that 51 percent of Irish-born men admitted to various psychiatric hospitals in New York had alcohol-related diagnoses, whereas only 4 percent of Italian-born men had similar diagnoses during the same period. Researchers identify two basic drinking patterns in European cultures: a Northern/Eastern European pattern(more common in the United States) in which alcohol is consumed only on weekends or during celebrations but often in large quantities on those occasions, and a Southern Europe pattern in which alcohol is consumed daily or almost daily but in smaller quantities and almost always with food (Room et al. 2003).White American men, on average, begin drinking and develop alcohol use disorders at a younger age than men from other racial/ethnic groups (HHS, SAMHSA, OAS 2008a;Reardon and Buka 2002). However, certain White American groups, (e.g., those of Middle Eastern descent) may drink very little if atall (Arfken et al. 2007). Hispanic/Latino AmericansWithin-group diversityHispanic and Latino are terms used to refer to cultures that originated, at least in part, in Spain or Portugal, and most often indicate people from Western Hemisphere cultures that have been influenced by Spanish or Portuguese colonization. The term Hispanic technically refers to people from the Spanish-speaking countries of North, Central, and South America and the Caribbean. However,the term Latino refers to people from Latin America, whether they are from a Spanish or Portuguese-speaking country. Unlike other groups described here, Hispanic/Latino is an ethnic, not a racial, category. Latinos may belong to any race and may include more than 30 national and cultural subgroups (Padillaand Salgado de Snyder 1992; Rodriguez-Andrew 1998). Latino Americans are currently the fastest-growing ethnic group in the United States (Ramirez and de la Cruz 2003; U.S. Census Bureau 2004).
[Question #76. Hispanic/Latino is anethnic, not a racial, category.] True/ False? Admission/substance use statisticsSAMHSA’s TEDS recognizes within-group diversity among Hispanics/Latinos by reporting admissions for diverse groups of Hispanicor Latino descent—the largest of these being Mexican and Puerto Rican. In the 2005 TEDS survey, Mexican American men made up 4.1 percent of treatment admissions; Puerto Rican men made up 3.2 percent of treatment admissions (SAMHSA, OAS 2008 b).
Data about drinking and drug use behaviors among various Hispanic/Latino groups, outside of those that enter treatment, do not always present a clear picture (Nielsen 2000).However, there seem to be significant variations in substance use patterns and disorders among diverse groups of Latinos (Alegria et al. 2008; HHS, SAMHSA, OAS 2000). Studies have consistently found that more acculturated Hispanics/Latinos drink more frequently and in larger quantities than less acculturated individuals (Alegria et al. 2008; Zemore 2005). Hispanic/Latino men are considered to be at high risk for alcohol abuse and dependence (Colon 1998; Corbett et al. 1991) and substance abuse (Vega et al. 1998). Among individuals entering substance abuse treatment,rates of heroin use are high for Puerto Rican men, as are rates of methamphetamine use for Mexican American men (Singer 1999). Geographic RegionsGeographic region can significantly affect the availability of substances, attitudes toward substance use, and cultural patterns of use for men. Each population has its own set of challenges that can contribute to the magnitude of substance use problems in that region. For example, men in rural settings may have less access to substance abuse prevention and treatment programs than men in urban settings but also less access to some illicit substances. Lo and Stephens (2002) compared arrestees’ perceived needs for substance-specific treatment in rural and urban settings.The investigators did not discuss gender other than to note that male detainees dependent on cocaine were less likely to express a need for treatment than female detainees dependent on cocaine. Nonetheless, they make some pertinent conclusions about urban/rural differences. As a general rule, urban arrestees were more likely to perceive a need for treatment and to exhibit increased motivation for treatment, whereas rural residents exhibited decreased motivation for treatment. More educated rural arrestees were less likely to be receptive to alcohol treatment than those who were less educated, whereas the converse was true in urban areas. The authors speculate that uneducated, unemployed rural residents stood the least to lose by entering treatment.
ConclusionBehavioral health programs and providers should consider the variety of factors that influence the significant disparity in substance use disorder rates between men and women in the United States. These factors range from greater opportunity to use substances to increased social pressure and possibly to a greater genetic disposition to use substances. In addition, men’s reasons for substance use differ from those of women and include rites of passage and a greater need to medicate feelings and emotions that they have difficulty expressing. The factors at work differ not only between genders, but also among men from diverse cultural and ethnic groups; providers need to consider these various and complex factors as they undertake the screening and assessment approaches outlined in Chapter 2.
|
|
|
Addressing Behavioral Health Needs of Men: Substance Abuse > Chapter 4 - Working With Specific Populations of Men in Behavioral Health Settings
Page Last Modified On: 18-Apr-2015 04:01 AM
|
|